
Designing for Wellness: Key Considerations for Healthcare Spaces in Justice Settings
Setting the Scene
If you have been around the corrections community long enough, you are aware of the challenges associated with overcrowding, aging infrastructure, and unconstitutional conditions associated with access to care for both mental and medical health needs. Many federal, state, and local municipalities are looking at how to approach upgrading and investing in new or existing facilities. The ongoing challenges related to deferred maintenance costs, an aging prison population, increasing demand for mental health treatment, drug abuse programs, and litigation associated with these and other matters are well documented and are resulting in a massive move to stabilize, revitalize, and even reinvent corrections to address these shortfalls. Almost every state in the country is working to address their specific needs. Healthcare is increasingly a larger component of the discussion, and much of what drives decision making is tied to the health and wellness of the inmate population and the patients that are currently being detained.
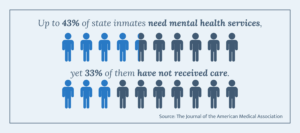
Nationwide, nearly two million people are confined across state and federal detention facilities, and local jails and prisons. The Office of the Assistant Secretary for Planning and Evaluation reports that close to seven million enter and exit these systems annually. The population of our prisons are aging and becoming sicker – according to the Prison Policy Initiative, between 40 and 60% of state inmates have chronic conditions. The mental health crisis in our prisons is also deepening. The Prison Policy Initiative cites up to 43% of state inmates need mental health services, yet 33% of them have not received care (JAMA).
It should also be noted the health and wellness of staff is an equally important consideration. Retention is a challenge for all organizations, and it is no different for corrections. Corrections officers and staff work in highly stressful environments, often working long hours with elevated levels of anxiety. Safety and security are essential but softening the environment ever-so-slightly can result in tangible health benefits for both inmates and staff, as well as provide lasting effects on job satisfaction and retention.
We know that many state-owned facilities still in use today are more than 80 years old, in disrepair, built with antiquated designs, and lack consideration for PREA or mental or physical health accommodations. For many in corrections, the healthcare elements paired with a shifting cultural mindset away from incarceration towards one of rehabilitation are foreign and often overwhelming. The new norm is to not only look at intake and housing but more importantly, the re-entry elements of reintroducing a previously incarcerated individual to society in a more positive and productive way.
So, Where Do We Start?
Correctional leaders and administrators may know they need to improve current healthcare conditions and access, sometimes by renovating an existing facility or building new. Beyond that, there may be a larger question mark around what remains with how to go about it and the things they need – including what services to provide, adequate space requirements, equipment needs, and soft design elements. Today’s blog post will help narrow the scope on this topic and boil the information down to provide some meaningful insight for designers, developers, and practitioners.
Here are a handful of recommendations to consider:
1. Design with a Purpose
What is the main goal of the facility you’re developing or renovating?
A foundational question architects must ask during project conception is: “Is this a hospital with added security, or a prison that happens to provide healthcare?” These opposing mindsets influence everything from spatial layout to patient flow, forensic design, and environmental features. A hospital-first approach prioritizes patient privacy, natural daylight, calming views, and rehabilitation-centric amenities.
A security-first approach tends to favor controlled sightlines, robustness, and minimal amenities, which often undermine therapeutic outcomes. Best-in-class designs harmonize both by integrating evidence-based healthcare design principles like single-bed rooms, natural light, clear wayfinding, and access to nature, while ensuring safety protocols are not compromised.
Did You Know?

Construction underway at the Governor Kay Ivey Correctional Institute (pictured above).
The Alabama Department of Corrections’ new Governor Kay Ivey Correctional Complex (“GKICC”) in Elmore County, Alabama is a new 4,000 bed facility that includes a centralized intake that will allow for significantly improved efficiencies. Inmates can be processed through intake, kept for treatment, or moved to other facilities if they do not have immediate medical needs. The State also will have the ability to look at classification levels of the current population and make quick and decisive moves to relocate someone at risk to the GKICC to receive care. The GKICC takes into consideration the safety and security associated with correctional environments but also addresses privacy, ADA requirements, and all the modern elements of a medical facility – including triage, diagnostics, emergency, dialysis, dental, vision, physical therapy, memory, geriatrics and mental health – to ensure those in their supervision have access to care and their needs are being met.
2. Identify Applicable Governance and Standards
What systems, processes, and institutions will you look to for guidance? What standards will be followed?
Whether a project be an intake center, specialized housing in a detention or a correctional environment, county facility or juvenile detention center, there are numerous factors to consider. National Commission on Correctional Health Care (NCCHC) standards for health services are an important resource and baseline to consider for any new project. The NCCH standards cover everything from governance, access to care, disease prevention, medication management, privacy, diets and transfers, safety, health services, and legal issues. Familiarity with these national standards will help to provide insight and guide discovery conversations when establishing design criteria, as well as with the finalization of design drawings and documents.
Early establishment of whether the authority will follow Joint Commission on Accreditation of Healthcare Organizations (JCAHO) public health standards or American Correctional Association (ACA) and NCCHC correctional healthcare standards will also aid with establishing criteria and specifications associated with HEPA filtration, medical gases and headwalls, as well as pharmacy and other needs and service lines. Upgrading to higher care standards not only supports Eighth Amendment protection but also controls long-term costs by improving chronic condition management.
Did You Know?
Healthcare is a costly endeavor. It is important to be explicit about medical gas requirements, headwall quantities, bed types, HEPA filtration, ADA equipment, AED locations for life safety plans, and WAP needs associated with communications and charting. Not establishing clear expectations in any of these categories could create downstream impacts that result in delays and significant additional cost associated with change orders.
3. Consider Your Stakeholders:
Who will be involved and impacted by this new or updated facility?

It’s vital to ensure there is a clear understanding of the vision of the project – the balance between custody and care, safety and security, and governance – and that lines of communication remain open. Doing so requires that you engage key stakeholders, specifically the healthcare teams, early and often. Make sure to also include input from community providers. Hold design sessions and town halls with correctional staff, healthcare providers, formerly incarcerated individuals, and community partners to align mission and human-centric needs with an evidence-based approach. A successfully executed project will require trusted advisors and industry partners, as well as contractors. Detailed timelines designed to achieve the undertaking of a large scale, multi-year, multimillion-dollar, complex project must also be clearly identified and used to set realistic expectations. As with most projects, open and effective lines of communication are key to success. Establishing proper distribution channels, milestones, meeting schedules, and informative Q&A sessions are also critical and should not be overlooked or taken for granted.
Did You Know?
Pharmaceutical medication management and dialysis are two specific areas that will require additional planning and foresight and must not be overlooked. State boards will need to be involved with the accreditation and activation of services. Setting meetings with stakeholders early in the process will help to avoid these types of blind spots that otherwise would inevitably occur. Healthcare practitioners are practical and logical with their approach – they know the nuances that exist state-to-state that are associated with their specialties.
4. Closely Review Clinical/Mental Health Considerations
What types of services, programming, and design elements should be incorporated in the facility?
A large part of scoping the project will require working with administrators and service providers to map out services, therapeutic programs, and equipment needs. However, the importance of therapeutic design elements should also be heavily considered. These elements, such as calming colors, natural light, outdoor views, sound attenuation, and access to secure outdoor spaces, have proven to reduce stress and the occurrence of aggressive incidents. Mental health clinics with private consult rooms, spaces for group therapy, and calming areas should be incorporated into the design criteria. Observation and isolation rooms should be designed to serve multiuse functions and telehealth spaces should be utilized to expand access and enable remote care. Applying evidence-based design elements and research-backed features – such as daylight optimization, reduced noise, and layouts that support safety and recovery – have been proven to reduce medical errors and enhance staff well-being.

The Hawaii Women’s Correctional Center (pictured above) utilizes outdoor spaces and cheerful colors to enrich their environment.
Integrating robust telecommunications infrastructure to support telehealth, remote court appearances, and virtual family visits is also an important consideration. Tablets in housing units increase family connection and enable remote therapy and educational programming linked to reduced infractions and stronger compliance. Facility Guidelines Institute’s (FGI) hospital guidelines should be utilized, directionally, for space minimums, and should be adjusted accordingly to account for a correctional context. ACA standards covering safety, care, programming, and security integration should be weighed more heavily for compliance.
Did You Know?
CDCR’s, California Health Care Facility (CHCF) in Stockton utilizes the painting of murals to help with the creation of calming environments, and Pennsylvania’s SCI Chester facility, otherwise known as “Little Scandinavia,” takes this approach one step further utilizing plants, fish tanks, furniture layout and communal cooking to enhance the process of rehabilitation.

Pictured above: California Health Care Facility (CHCF)
5. Prioritize Reentry & Continuity of Care (CoC)
What considerations must be made to keep reentry and CoC needs top of mind?
To meet the increasing need for planning and coordination associated with reentry and continuity of care for inmates, clinics and multipurpose rooms should be designed for reentry workshops, community provider visits, and telehealth sessions leading up to release. While undoubtedly institutional by necessity, the design of these areas should also aid in helping to facilitate handoffs to community providers. Consider secure digital health records, in-reach space for parole officers, job fairs, and housing providers, with the intent to allow for early access to medical evaluation and mental health planning – all of which has been shown to improve outcomes and reduce recidivism rates.
Did You Know?
Wake County’s evaluation of its Detention Medical Services Division identified key improvements that can generate cost savings without compromising care quality. These savings could be redirected to expand critical reentry supports, such as mental health continuity of care, jail diversion programs, and discharge medication management, enhancing detainees’ stability, treatment adherence, and access to services upon release.
The End Goal: Designing for Transformation
Well-designed correctional healthcare environments do more than meet minimum standards, they transform them – improving health, reducing recidivism, strengthening reentry, and supporting staff. By embracing the lenses of healthcare, therapeutic design, and technology, and forging strong ties with community providers, designers can lead the shift from walls of confinement to pathways of rehabilitation and reintegration.
Meet the Author



